Planning for failure: The key to success
Airway management is dangerous. This is particularly true of emergency airway management in the ED or ICU. Our environment is often uncontrolled and our patients often have hemodynamic or respiratory compromise which significantly increases the risk of intubation. Moreover, although many tools exist to help predict a difficult airway, none are perfect and as such a difficult airway may present without warning. For these reasons we need to approach EVERY airway as a potentially difficult airway and articulate a clear plan for failed intubation and failed oxygenation.
Failure to plan for failure and repeated laryngoscopy attempts despite failure have been identified as common critical errors leading to morbidity and mortaliaty by the 4th National Audit Project (NAP4): Major complications of airway management in the United Kingdom. The link is for the summary document which is only 3 pages, it is a ‘must read’ paper. The full report is over 200 pages and only for the truly dedicated!
In the previous post I discussed the importance of cognitive readiness for all members of the team. In this post I would like to introduce a cognitive tool for airway management which helps team members share a mental model in the event of difficulty securing the airway. Plastic in the trachea is NOT the goal. Our aim is preservation of oxygenation and hemodynamics by whatever means necessary.
The Vortex is a “high stakes cognitive aid” for airway management. It aims to train staff for management of the unanticipated difficult airway using a single simple & universally applicable template that is taught to ALL staff likely to be involved in managing the crisis (medical, nursing, RT etc).
This video provides a brief introduction to the Vortex approach. You can also download the complete free ebook for a more detailed discussion.
This video outlines the use of the Vortex approach in a simulated ED scenario
The centre of the vortex is the emergency surgical aiway (ESA) or crycothyroidotomy. This approach requires readiness for ESA at EVERY intubation. This is also in keeping with the findings of NAP4 that surgical airway was often performed late or not at all. Nicholas Chrimes, creator of the Vortex approach has simplified Scott Weingart’s Cric Con concept in an attempt to help overcome the psychological & practical hurdles of deciding to “cut the neck. If preparation for initiating ESA has not been made in advance of the decision to perform it, the delays can be surprisingly long which may expose the patient to critical hypoxia.
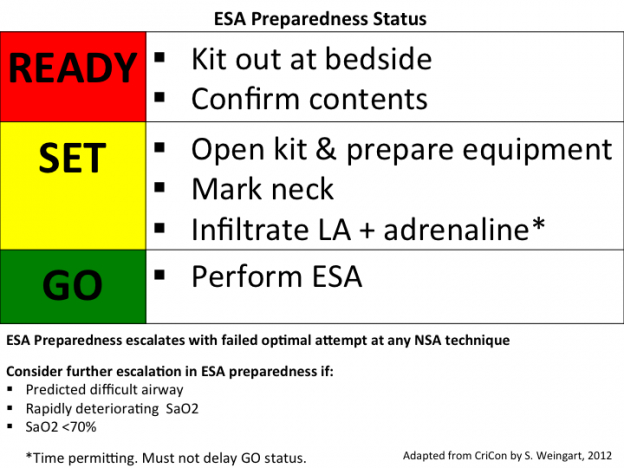
A declared failure of an optimal attempt at any non surgical airway technique (ETT, LMA, BMV) mandates an escalation in ESA preparedness by the team. Sequential failure of optimal attempts at all three NSA techniques will therefore place airway management teams at “GO” status as they enter the ESA portion of the Vortex, having already prepared the necessary equipment during the “READY” and “SET” phases.
I like the Vortex approach for it’s simplicity but it does require a certain degree of training to get used to it. However, regardless of whether you decide to adopt the Votex approach in your practice the key message cannot be ignored.
- PREPARE FOR FAILURE – be ready for ESA at EVERY intubation
- No more than 3 attempts at any non surgical airway technique
- Optimize between each attempt (manipulations/adjunct/device etc.)
- Communicate with your team – Verbalize Plan A, B & C
If the team plans for difficulty before every intubation it is far more likely that they will be able to respond appropriately when real difficulty arises.

thank you Scott,i like the Vortex approach and in was waiting for sothing realy simple that every body taking care of airway can do it and i think it is this approach . what we need is to make every body familiar with it ,and make it as habit and routine